

Curriculum - Great Vessels
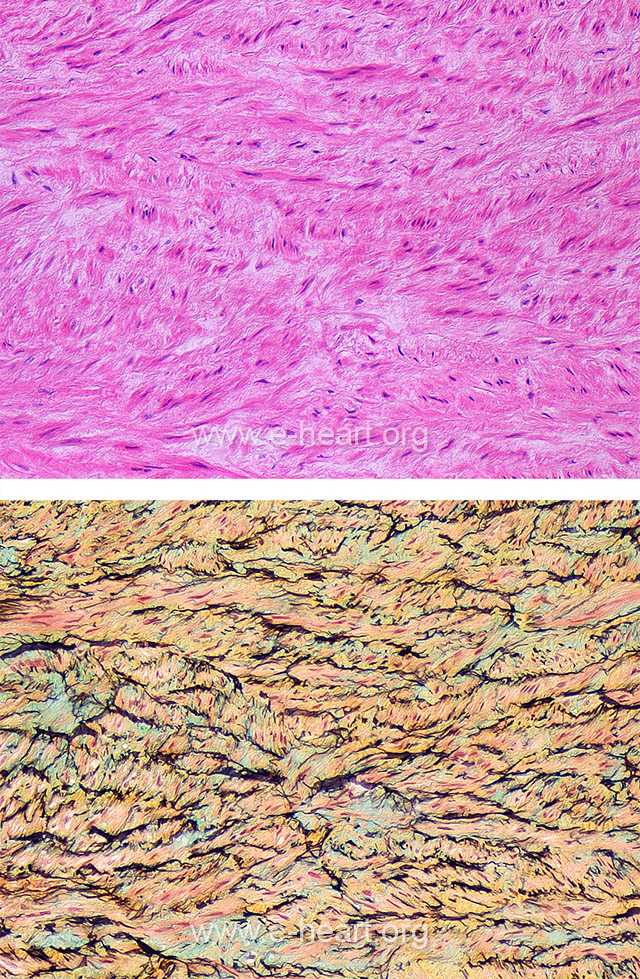
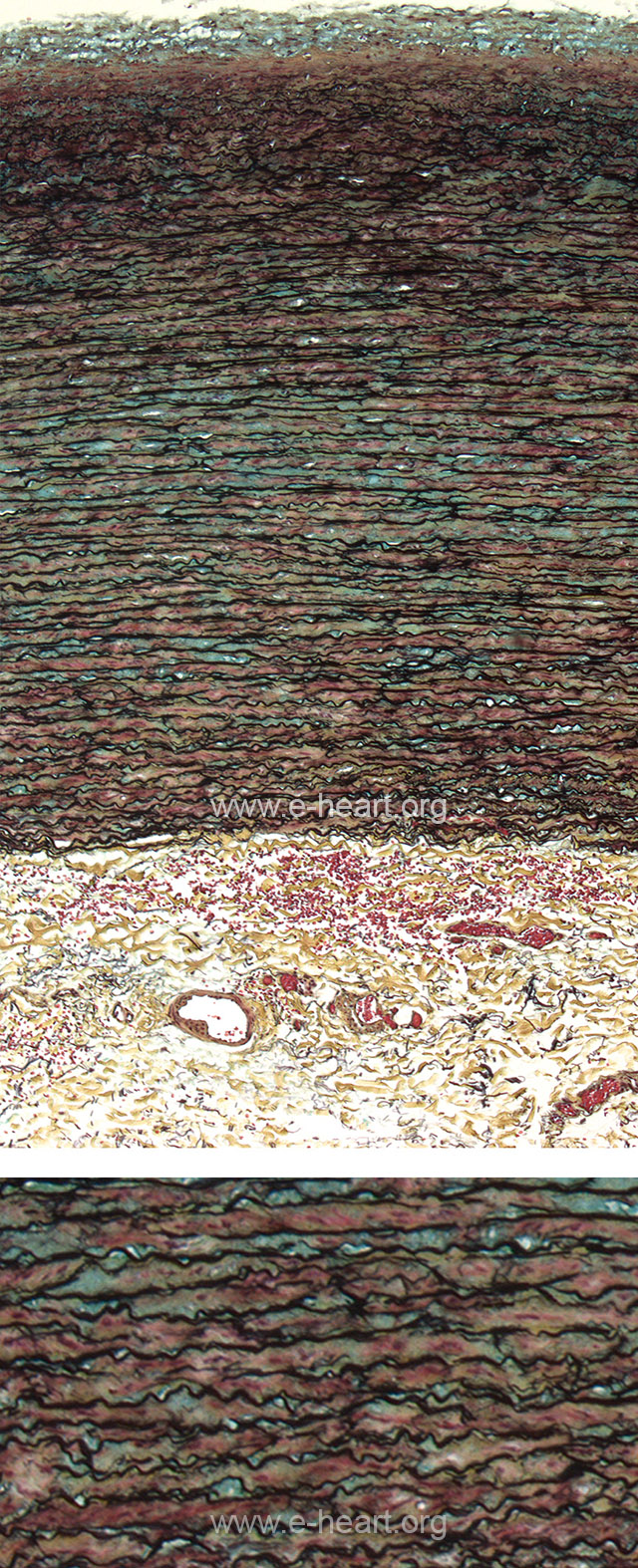 Elastic type arteries, like any other type of arteries have a tunica intima, a tunica media and a tunica adventitia (upper image). The distinguishing architectural feature of an elastic type artery is that it is composed of lamellar units. The components of the lamellar unit are two elastic lamellae containing a small amount of fibrous tissue and mucopolysaccharide synthetized by smooth muscle cells in the middle of the lamellar unit (lower image). The aorta has approximately 40 lamellar units in the ascending portion which progressively diminish distally, with only about 20 lamellar units in the lower abdominal aorta. The elastic arteries in the body include aorta, carotids, subclavian, iliacs and some branches from these. In addition the pulmonary artery is also an elastic-type artery. Vasa vasorum are prominent in the adventitia and rarely penetrate into the media unless there are pathologic changes in the arterial wall.
Elastic type arteries, like any other type of arteries have a tunica intima, a tunica media and a tunica adventitia (upper image). The distinguishing architectural feature of an elastic type artery is that it is composed of lamellar units. The components of the lamellar unit are two elastic lamellae containing a small amount of fibrous tissue and mucopolysaccharide synthetized by smooth muscle cells in the middle of the lamellar unit (lower image). The aorta has approximately 40 lamellar units in the ascending portion which progressively diminish distally, with only about 20 lamellar units in the lower abdominal aorta. The elastic arteries in the body include aorta, carotids, subclavian, iliacs and some branches from these. In addition the pulmonary artery is also an elastic-type artery. Vasa vasorum are prominent in the adventitia and rarely penetrate into the media unless there are pathologic changes in the arterial wall.
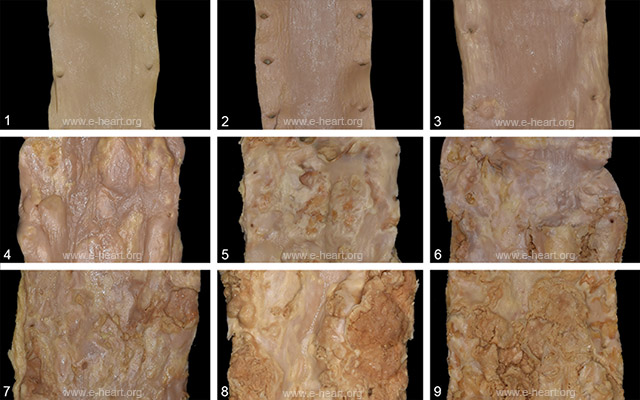 Atherosclerosis in the aorta is a progressive disease. This panel show the intima of thoracic aortae. 1. Normal aorta without atherosclerosis. 2. Early fatty streaks in the intima run parallel to the axis of the artery. 3. The fatty streaks are more prominent raising above the surface of the intima. 4 – 6. Atheromatous plaque grow in size and coalesce to cover the entire surface of the vessel. Fibrous caps are cover the atheroma in a continuous fashion. However the lesions in image number 6 begin to show defects on the intimal surface. 7. The defects on the surface ulcerate and thrombose. 8-9. Further ulceration and thrombosis form complex plaques.
Atherosclerosis in the aorta is a progressive disease. This panel show the intima of thoracic aortae. 1. Normal aorta without atherosclerosis. 2. Early fatty streaks in the intima run parallel to the axis of the artery. 3. The fatty streaks are more prominent raising above the surface of the intima. 4 – 6. Atheromatous plaque grow in size and coalesce to cover the entire surface of the vessel. Fibrous caps are cover the atheroma in a continuous fashion. However the lesions in image number 6 begin to show defects on the intimal surface. 7. The defects on the surface ulcerate and thrombose. 8-9. Further ulceration and thrombosis form complex plaques.
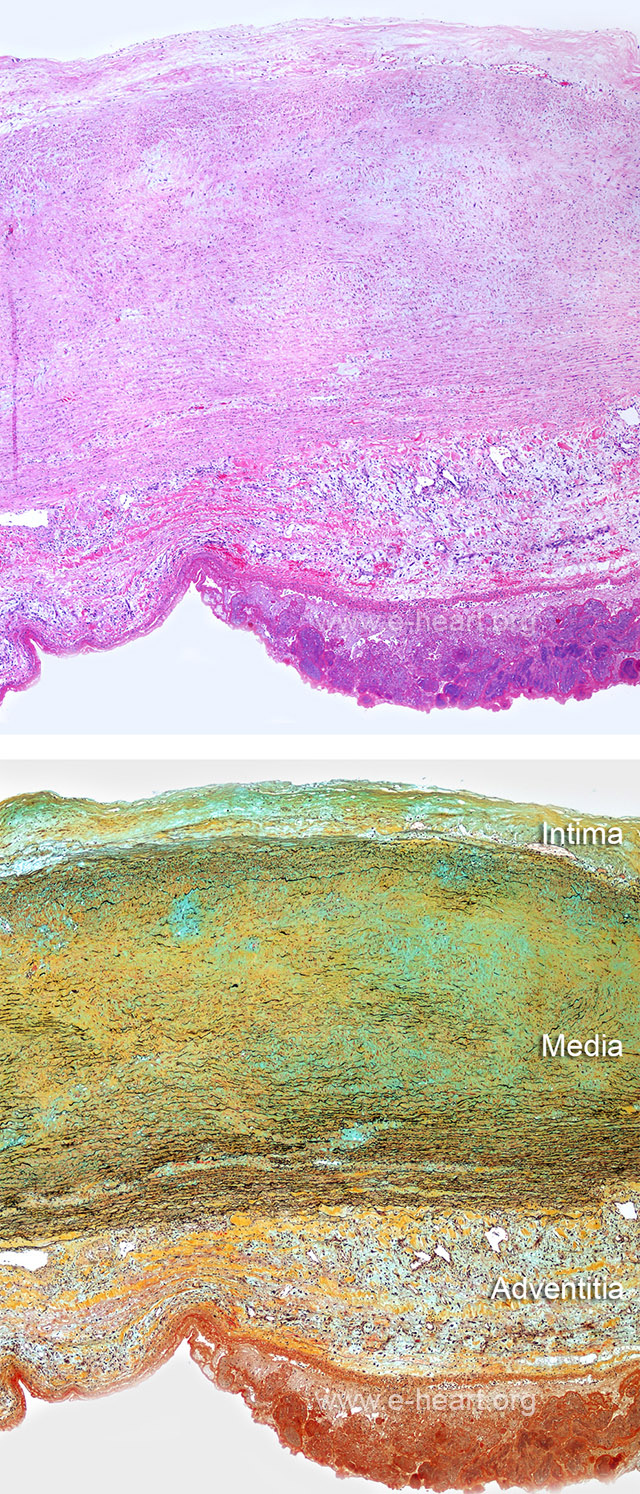 Cystic medial degeneration of the aorta. This is not a necrotizing process of smooth muscle cells. Instead it is a degenerative process the affects the elastic lamellae of the aorta. It is an interruption of the parallel array of elastic laminae (black lines, compare to Figure 27.72). This interruption creates areas devoid of elastic lamellae, thus giving an impression that a “cyst” in the parallel pattern of lamellae has formed. The Movat stain (lower image) show these areas clearly. They show fibrous tissue (yellow) and can show large pools of mucopolysaccharide / proteoglycan material. This change is non-specific and can be seen in aneurysms with a clear genetic basis as well as in atherosclerosis.
Cystic medial degeneration of the aorta. This is not a necrotizing process of smooth muscle cells. Instead it is a degenerative process the affects the elastic lamellae of the aorta. It is an interruption of the parallel array of elastic laminae (black lines, compare to Figure 27.72). This interruption creates areas devoid of elastic lamellae, thus giving an impression that a “cyst” in the parallel pattern of lamellae has formed. The Movat stain (lower image) show these areas clearly. They show fibrous tissue (yellow) and can show large pools of mucopolysaccharide / proteoglycan material. This change is non-specific and can be seen in aneurysms with a clear genetic basis as well as in atherosclerosis.
 Gross specimen showing a a posterior view of an aortic dissection. A type “A” dissection occurred in the past and was repaired by replacing the ascending aorta with a Dacron graft. Another dissection (Type B) extending from just beyond the left subclavian. The inset shows the new intimal tear (IT) the true lumen (T) and the false lumen (F) of the dissected aorta.
Gross specimen showing a a posterior view of an aortic dissection. A type “A” dissection occurred in the past and was repaired by replacing the ascending aorta with a Dacron graft. Another dissection (Type B) extending from just beyond the left subclavian. The inset shows the new intimal tear (IT) the true lumen (T) and the false lumen (F) of the dissected aorta.
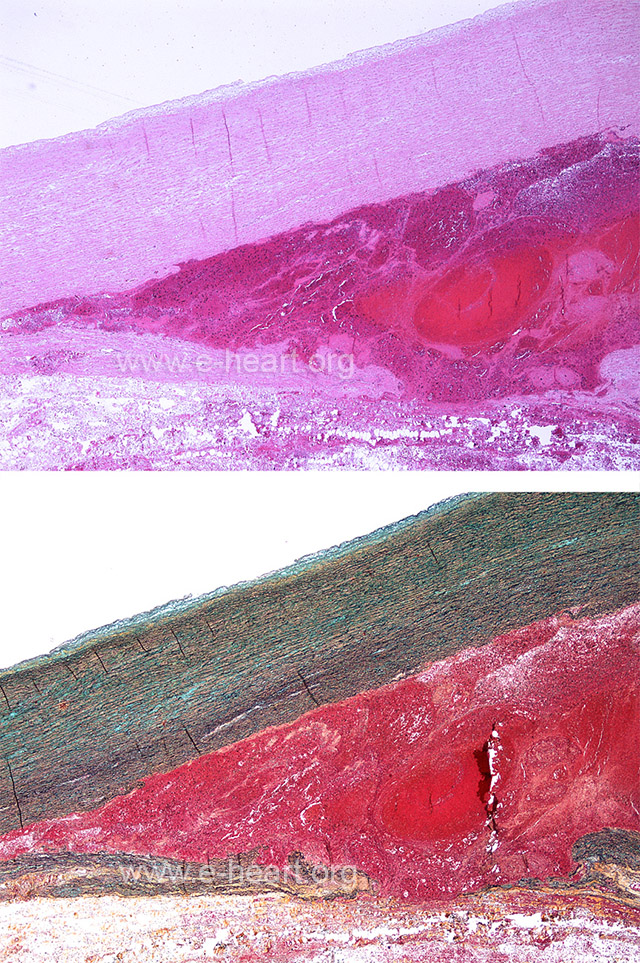 Acute aortic dissection. The media of the aorta shows a dissection plane filled with blood which is extravasating into the adventitia.
Acute aortic dissection. The media of the aorta shows a dissection plane filled with blood which is extravasating into the adventitia.
 Aortic wall with marked disarray of the smooth muscle bundles. Despite correct orientation of the sample, the circular array of smooth muscle cells is lost. The Movat stain also shows a rather disarrayed organization of the elastic lamellae, which are no longer parallel.
Aortic wall with marked disarray of the smooth muscle bundles. Despite correct orientation of the sample, the circular array of smooth muscle cells is lost. The Movat stain also shows a rather disarrayed organization of the elastic lamellae, which are no longer parallel.
 Posterior view of the thoracic aorta with a fusiform aneurysm starting in the aortic arch.
Posterior view of the thoracic aorta with a fusiform aneurysm starting in the aortic arch.
 Takayasu arteritis. The H&E stain shows very thick adventitia and intima layers with a somewhat thinned media. There is inflammatory infiltrate visible in the media and adventitia. The media shows collapse and partial destruction of the elastic lamellae. The intima shows an exuberant
Takayasu arteritis. The H&E stain shows very thick adventitia and intima layers with a somewhat thinned media. There is inflammatory infiltrate visible in the media and adventitia. The media shows collapse and partial destruction of the elastic lamellae. The intima shows an exuberant
“neointima” with dense fibrous tissue as well as proteoglycan-rich connective tissue. The insets on the right panels show higher magnification with mononuclear inflammation and giant cells both on the H&E and the Movat stain.
 On gross exam the arteries with Takayasu’s disease show marked thickening of the vessel wall because this entity is commonly a pan-arteritis affecting the adventitia, media and intima of the vessel. The inflammatory infiltrates and the extracellular matrix response to the inflammatory insult produce thickening of the adventitia and intima and to some extent thinning of the medial. For comparison a normal thoracic aorta is shown, where the intima and adventitia are thin and most of the wall thickness represents the media.
On gross exam the arteries with Takayasu’s disease show marked thickening of the vessel wall because this entity is commonly a pan-arteritis affecting the adventitia, media and intima of the vessel. The inflammatory infiltrates and the extracellular matrix response to the inflammatory insult produce thickening of the adventitia and intima and to some extent thinning of the medial. For comparison a normal thoracic aorta is shown, where the intima and adventitia are thin and most of the wall thickness represents the media.
 Luminal view of an aorta with severe atherosclerosis with complicated ulcerated plaques forming a saccular aneurysm, which, in turn, is filled with thrombus.
Luminal view of an aorta with severe atherosclerosis with complicated ulcerated plaques forming a saccular aneurysm, which, in turn, is filled with thrombus.
 Giant cell aortitis, in comparison to Takayasu’s disease (Figure 27.88) shows a rather white intima with some “tree barking” alternating with yellowish areas (see microscopic image in Figure 27.93). On cross section the relative thickness of the intima media and adventitia is similar in the three layers. The aorta with giant cell arteritis is only slightly thicker than the normal aorta shown in the bottom part.
Giant cell aortitis, in comparison to Takayasu’s disease (Figure 27.88) shows a rather white intima with some “tree barking” alternating with yellowish areas (see microscopic image in Figure 27.93). On cross section the relative thickness of the intima media and adventitia is similar in the three layers. The aorta with giant cell arteritis is only slightly thicker than the normal aorta shown in the bottom part.
 Microscopic examination shows a proliferative intima. The media shows large areas of laminar necrosis (i.e. necrosis of the smooth muscle, without disappearance of the elastic lamellae, which instead collapse. Proliferation of vasa vasorum from the adventitia into the middle third of the media is common. The inflammatory infiltrates (mononuclear cells and giant cells) are commonly found in the vicinity of these vasa vasorum (insets H&E and Movat).
Microscopic examination shows a proliferative intima. The media shows large areas of laminar necrosis (i.e. necrosis of the smooth muscle, without disappearance of the elastic lamellae, which instead collapse. Proliferation of vasa vasorum from the adventitia into the middle third of the media is common. The inflammatory infiltrates (mononuclear cells and giant cells) are commonly found in the vicinity of these vasa vasorum (insets H&E and Movat).
 The intima in giant cell aortitis shows exuberant proteoglycan-rich extracellular matrix. In this example the destruction of the media has produced distinct collapse of the elastic lamellae of the media or complete disappearance of the elastic lamellae as the process heals. The adventitia is slightly thickened by dense fibrous tissue, but no giant cells or granulomata are present, in contrast to Takayasu’s disease.
The intima in giant cell aortitis shows exuberant proteoglycan-rich extracellular matrix. In this example the destruction of the media has produced distinct collapse of the elastic lamellae of the media or complete disappearance of the elastic lamellae as the process heals. The adventitia is slightly thickened by dense fibrous tissue, but no giant cells or granulomata are present, in contrast to Takayasu’s disease.
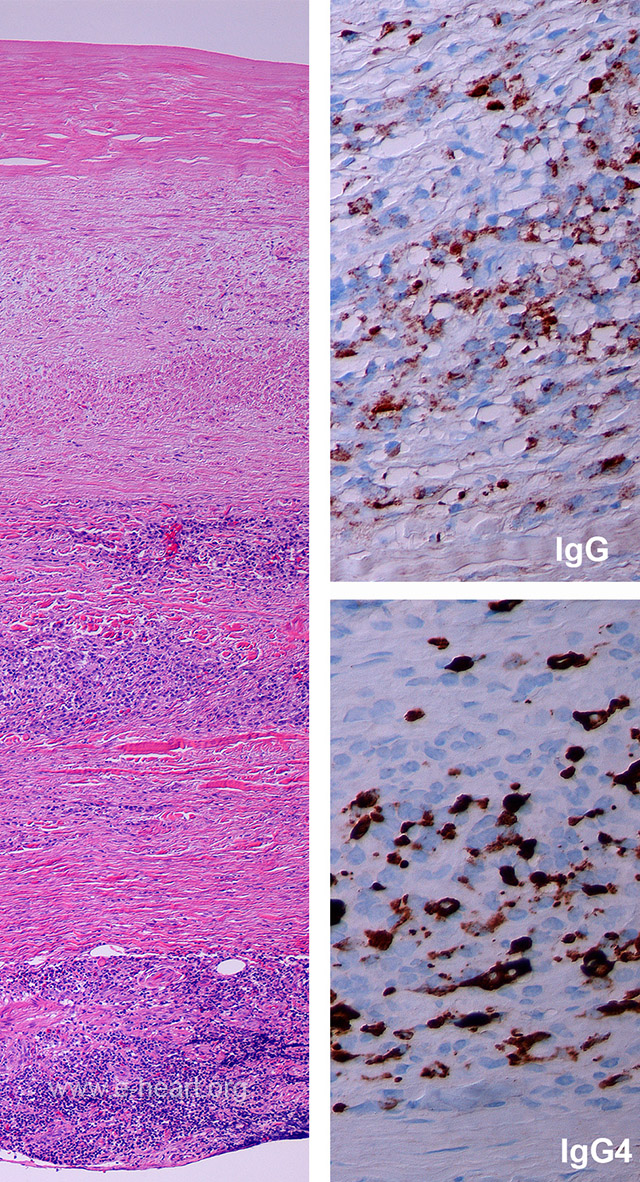 Arteritis of the aorta showing prominent plasma cell populations in the inflammatory infiltrate should be evaluated for immunoglobulin subtypes produced by the plasma cells. If greater than 50% of all the plasma cells stain with IgG4 antibody, the diagnosis of IgG4 related disease can be rendered. The panels on the right show that a little over 50% of the plasma cells expressing immunoglobulin also express IgG4.
Arteritis of the aorta showing prominent plasma cell populations in the inflammatory infiltrate should be evaluated for immunoglobulin subtypes produced by the plasma cells. If greater than 50% of all the plasma cells stain with IgG4 antibody, the diagnosis of IgG4 related disease can be rendered. The panels on the right show that a little over 50% of the plasma cells expressing immunoglobulin also express IgG4.
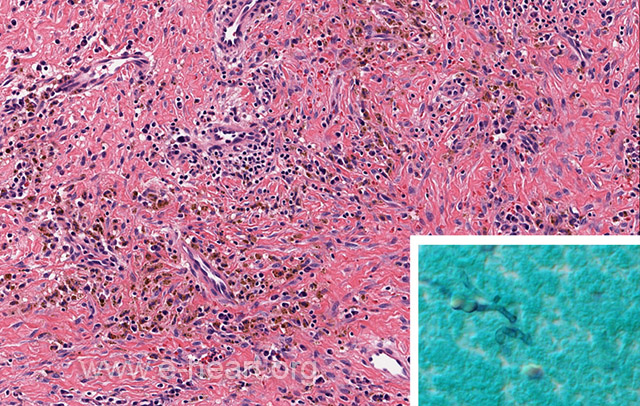 The wall of this mycotic aneurysm shows dense reactive fibrous tissue and chronic inflammation as well as hemosiderin laden macrophages. The GMS stain show very fain fungal hyphae.
The wall of this mycotic aneurysm shows dense reactive fibrous tissue and chronic inflammation as well as hemosiderin laden macrophages. The GMS stain show very fain fungal hyphae.